Mesothelioma survival rates describe outcomes among groups of people diagnosed with this rare cancer. They can provide useful context after a diagnosis, but they cannot predict exactly how long any individual person will live.
Survival varies considerably. The location of the cancer, extent of disease, tumor histology, age, overall health, functional status, and available treatment options can all influence prognosis. Outcomes reported in historical datasets may also differ from those of people receiving newer therapies today.
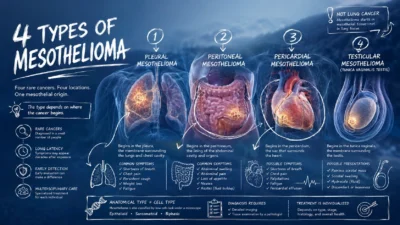
Mesothelioma is a cancer of the mesothelium, the thin tissue that lines and protects several internal organs. Most cases arise in the pleura, the lining around the lungs. Mesothelioma can also develop in the peritoneum surrounding abdominal organs and, much more rarely, in other mesothelial tissues.
Asbestos exposure is the primary established risk factor for malignant mesothelioma. The disease often develops decades after exposure, contributing to the difficulty of recognizing it early.
What Are Mesothelioma Survival Rates?
A survival rate estimates the proportion of people with a particular cancer who remain alive for a defined period after diagnosis. Five-year survival is commonly reported, although one-year and three-year outcomes may also appear in research and cancer statistics.
One important distinction is between overall survival and relative survival.
Overall survival measures the proportion of patients who remain alive after a specified period, regardless of cause of death. Relative survival compares survival among people with cancer with the expected survival of people of similar age, sex, and other demographic characteristics in the general population.
This distinction matters when comparing statistics from different sources. A five-year overall survival figure and a five-year relative survival figure are not necessarily measuring the same outcome.
Survival statistics also describe populations rather than individuals. They are most useful for understanding broad patterns, comparing groups, and supporting discussions about prognosis. They cannot account for every feature of an individual case.
Current Survival Statistics for Pleural Mesothelioma
Pleural mesothelioma is the most common form of the disease and has the most extensive population-level survival data.
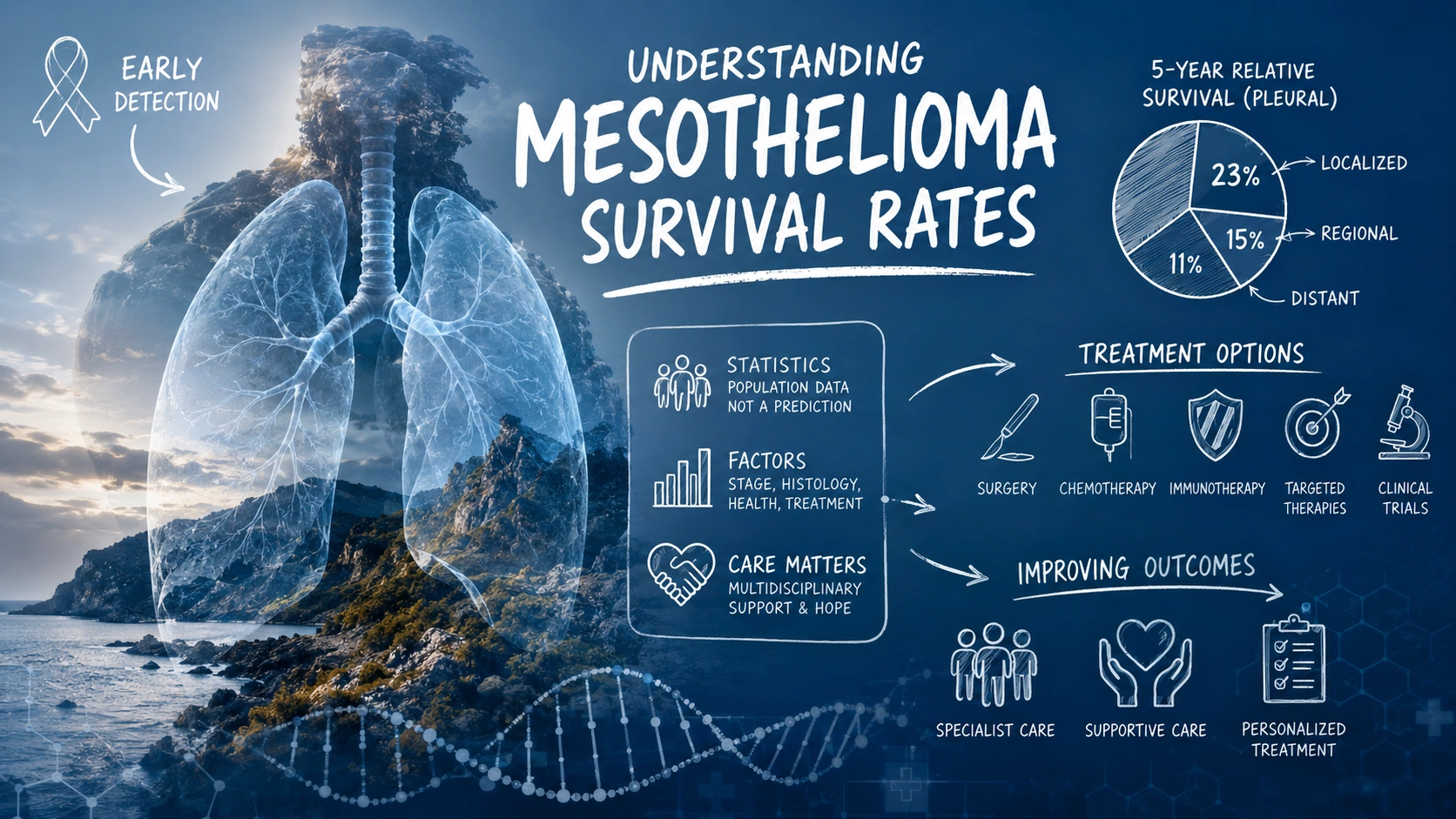
According to American Cancer Society data based on people diagnosed with pleural mesothelioma from 2015 through 2021, five-year relative survival rates were:
SEER stage 5-year relative survival Localized 23% Regional 15% Distant 11% All stages combined 15%
These figures should be interpreted carefully.
The Surveillance, Epidemiology, and End Results (SEER) system uses the categories localized, regional, and distant. These categories are broader than the stage I–IV system commonly used in clinical discussions of pleural mesothelioma.
Survival data are also retrospective. People included in a survival dataset were diagnosed years earlier, meaning the statistics may not fully capture the effects of treatments introduced or adopted more recently.
For that reason, population survival figures are best viewed as a reference point rather than a personal prediction.
Why Mesothelioma Survival Rates Differ Between People
Two people with mesothelioma can have substantially different outcomes even when their diagnoses initially appear similar. Prognosis reflects a combination of tumor characteristics, disease extent, general health, and treatment-related factors.
The following are among the most important considerations.
1. Stage and Extent of Disease
Cancer stage describes how far a tumor has grown or spread. In general, disease confined to a smaller area is associated with better survival than cancer that has extensively invaded surrounding structures or spread to distant sites.
Pleural mesothelioma is commonly described using stages I through IV:
- Stage I: Disease is relatively localized to one side of the chest.
- Stage II: The cancer has extended into additional nearby structures and may involve regional lymph nodes, depending on the precise staging classification.
- Stage III: The tumor is more locally advanced and may involve additional structures or lymph nodes.
- Stage IV: Disease is extensively advanced or has spread to distant parts of the body.
The exact clinical meaning of a stage depends on the staging system and tumor characteristics. Staging is therefore more complex than a simple progression from one isolated layer of tissue to another.
Earlier-stage disease may create more opportunities for selected local treatment strategies, including surgery in carefully evaluated patients. However, stage alone does not determine treatment eligibility or prognosis.
Histology, overall health, functional status, tumor distribution, and whether the disease can be removed surgically also influence treatment planning.
2. Mesothelioma Location
The anatomical site where mesothelioma begins affects both treatment strategy and prognosis.
Pleural Mesothelioma
Pleural mesothelioma develops in the tissue surrounding the lungs. It accounts for most mesothelioma cases and has established staging systems and several systemic treatment options.
Prognosis varies widely according to stage, histologic subtype, overall health, and treatment eligibility.
Peritoneal Mesothelioma
Peritoneal mesothelioma develops in the lining of the abdominal cavity.
Its prognosis should not be assumed to be worse than pleural mesothelioma simply because it occurs at a different site. Selected patients with disease suitable for aggressive regional treatment may undergo cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (HIPEC), although eligibility depends on individual clinical factors and specialist evaluation.
Because peritoneal mesothelioma is rare and treatment populations are highly selected, survival figures from individual treatment centers should not automatically be generalized to every patient.
Pericardial and Testicular Mesothelioma
Mesothelioma of the pericardium and tunica vaginalis of the testis are extremely rare.
Their rarity means survival estimates are based largely on small case series, retrospective analyses, and individual reports. Broad survival percentages for these cancers should therefore be interpreted cautiously.
3. Histologic Subtype
Histology describes how cancer cells look under a microscope. Mesothelioma is generally classified into three major histologic patterns:
- Epithelioid
- Sarcomatoid
- Biphasic, containing both epithelioid and sarcomatoid components
Histologic subtype is an important prognostic factor. Epithelioid mesothelioma generally has a more favorable prognosis than sarcomatoid disease. Biphasic tumors have mixed characteristics, and their behavior can vary.
Histology may also affect treatment decisions. For this reason, an accurate pathological diagnosis is a central part of evaluating a mesothelioma case.
4. Age, General Health, and Performance Status
Age can be associated with prognosis, but chronological age alone does not determine whether someone can receive a particular treatment.
Clinicians also evaluate factors such as:
- cardiovascular and respiratory function;
- kidney and liver function;
- other medical conditions;
- nutritional status;
- ability to perform normal daily activities;
- anticipated ability to tolerate treatment.
Performance status is particularly important in oncology. It describes how well a person can carry out ordinary activities and is frequently considered when selecting treatment and estimating prognosis.
A younger person may be able to tolerate intensive treatment more easily, but treatment decisions should be based on comprehensive clinical assessment rather than age alone.
5. Treatment Eligibility and Response to Therapy
Treatment can influence survival, but comparisons between treatment groups require caution.
People selected for surgery or intensive multimodal treatment may already have characteristics associated with a better prognosis, such as limited disease, favorable histology, stronger performance status, or fewer serious medical conditions. This selection effect makes it difficult to attribute differences in survival entirely to one treatment.
Mesothelioma treatment may include:
- surgery;
- chemotherapy;
- immunotherapy;
- radiation therapy;
- combinations of treatments;
- symptom-directed and palliative interventions;
- participation in clinical trials.
The appropriate strategy depends on the location and extent of disease, histology, symptoms, previous treatments, general health, and individual treatment goals.
How Mesothelioma Treatment Has Changed
The treatment landscape for malignant pleural mesothelioma has evolved substantially.
For many years, platinum-based chemotherapy combined with pemetrexed was a major systemic treatment approach. Immunotherapy has since expanded first-line options for unresectable disease.
The combination of nivolumab and ipilimumab is an established first-line immunotherapy option for unresectable malignant pleural mesothelioma in appropriate patients. Clinical evidence demonstrated improved overall survival compared with chemotherapy in the pivotal study population, although benefits and adverse effects vary between individuals.
In September 2024, the U.S. Food and Drug Administration also approved pembrolizumab in combination with pemetrexed and platinum chemotherapy for first-line treatment of unresectable advanced or metastatic malignant pleural mesothelioma.
These developments are important when interpreting older survival statistics. Population datasets necessarily look backward, while clinical practice continues to change.
Treatment selection remains individualized. Immunotherapy is not appropriate for every person, and immune-related adverse effects can affect multiple organ systems. Decisions should be made with an oncology team familiar with the patient’s disease characteristics and overall health.
Can Early Detection Improve Mesothelioma Survival?
Earlier-stage disease is generally associated with better survival, but the idea of “early detection” requires careful context in mesothelioma.
There is currently no established routine population screening program proven to reduce mesothelioma mortality. Even among people with a history of asbestos exposure, surveillance strategies require individualized medical evaluation.
Mesothelioma can also be difficult to diagnose because early symptoms may resemble more common conditions.
Depending on tumor location, symptoms can include shortness of breath, chest pain, persistent cough, abdominal swelling, abdominal pain, or unexplained weight loss. These symptoms have many possible causes and do not necessarily indicate mesothelioma.
People with a history of asbestos exposure should make sure their healthcare professionals know about that exposure history. New or persistent symptoms should be medically evaluated rather than attributed to mesothelioma without diagnostic testing.
Does Specialist Care Matter?
Mesothelioma is rare, and diagnosis and treatment can involve complex decisions across several medical specialties.
A multidisciplinary team may include:
- medical oncologists;
- thoracic surgeons or surgical oncologists;
- radiation oncologists;
- pathologists;
- radiologists;
- pulmonologists;
- palliative care specialists;
- oncology nurses and other supportive care professionals.
Evaluation at a center experienced in mesothelioma may provide access to specialized pathology review, multidisciplinary treatment planning, complex procedures, and appropriate clinical trials.
This does not mean that every patient must receive every available treatment. The value of specialist assessment lies in determining which options are appropriate for a particular case.
Clinical Trials and Mesothelioma Survival
Clinical trials evaluate new treatment strategies or new uses and combinations of existing therapies.
Depending on the trial, research may investigate:
- new immunotherapy combinations;
- targeted approaches for molecularly defined tumors;
- novel drug-delivery strategies;
- combinations of systemic and local therapies;
- biomarkers that may predict treatment response;
- treatment sequencing.
Participation in a clinical trial does not guarantee a better outcome. Trials have specific eligibility criteria, and experimental treatments may not prove more effective than existing care.
However, discussing clinical trials can be appropriate, particularly for a rare cancer in which treatment options and evidence continue to evolve.
Supportive and Palliative Care
Survival is only one part of mesothelioma care. Symptom control and quality of life also matter from the time of diagnosis.
Supportive and palliative care may help address:
- pain;
- shortness of breath;
- pleural or abdominal fluid accumulation;
- fatigue;
- appetite and nutrition concerns;
- anxiety and emotional distress;
- sleep problems;
- practical and caregiver needs.
Palliative care is not limited to the final stage of illness. It can be provided alongside cancer-directed treatment and adjusted as symptoms and goals change.
Procedures to manage recurrent pleural or abdominal fluid may also reduce symptoms in selected patients. The appropriate approach depends on where fluid is accumulating, how quickly it returns, and the person’s overall condition.
How to Interpret a Personal Prognosis
A population survival percentage cannot answer the question, “How long will I live?”
A more useful discussion with a medical team may consider:
- Where did the mesothelioma begin?
- What is the exact stage or extent of disease?
- What is the histologic subtype?
- Is the disease considered resectable or unresectable?
- What is the person’s performance status?
- Which treatments are medically appropriate?
- What are the goals and expected benefits of treatment?
- Are relevant clinical trials available?
- Which symptoms require immediate management?
- How might treatment benefits be balanced against potential adverse effects and quality of life?
Even then, prognosis remains an estimate. Some people live considerably longer or shorter than population averages.
The Bottom Line
Mesothelioma remains a serious and aggressive cancer, but survival statistics require careful interpretation.
For pleural mesothelioma, contemporary population data show better five-year relative survival for localized disease than for regional or distant disease. Stage, however, is only one part of prognosis. Histology, tumor location, overall health, performance status, treatment eligibility, and response to therapy can all influence outcomes.
Treatment has also changed. Modern immunotherapy regimens and newer combinations have expanded options for some people with unresectable malignant pleural mesothelioma, making older survival figures less representative of every person receiving treatment today.
The most useful prognosis comes from an individualized assessment based on pathology, staging, overall health, and current treatment options. People diagnosed with mesothelioma may benefit from multidisciplinary evaluation and, when appropriate, discussion of clinical trials and early supportive care.
- About the Author
- Latest Posts

Salwa Alifah Yusrina is the Editor-in-Chief at Medslat.com. She is a professional Nutritionist with over 7 years of clinical and research experience. She holds a Master’s degree in Nutrition Science from Hasanuddin University. At Medslat.com, she oversees the editorial direction and ensures that all health and nutrition content adheres to the highest standards of accuracy and evidence-based science.